For me, the worst part of gastritis was never the burning.
It was the nausea. The anxiety that seemed to arrive from nowhere. The weeks where I could barely get myself to eat anything, even though I knew eating was the only way to stop feeling so sick. And the depression – dark room, no energy, no serotonin, no idea how I was going to get through the next flare.
I am a certified holistic nutritionist. I have had chronic gastritis for ten years. And I spent years convinced I had a separate anxiety problem on top of the gastritis. I didn’t. I had gastritis. The anxiety was part of it. So was the nausea, the eating problem, and the depressed mood. They were all coming from the same place.
The reason nobody warned me is that most gastritis content focuses on stomach pain and food triggers. Those are real. They are also only part of the picture. This post covers the four symptoms that the standard medical content almost never discusses: nausea, anxiety, the eating problem during flares, and the depression that follows. If you have any of them, you are going to read your own experience back to yourself here.
The nausea that won’t quit
Gastritis nausea is not the kind that comes right before you are sick and then resolves. It is ambient. A low-grade queasy, on-edge feeling that can last for days or weeks, sometimes with no connection to a specific meal. Morning nausea. Nausea during stress. Nausea that arrives without a trigger and sits there, making everything harder.
The mechanism is straightforward but rarely explained. When the stomach lining is inflamed, the stomach’s normal motility patterns are disrupted. Gastric emptying slows. Food that should move through in a predictable pattern lingers. The stomach fills faster, empties later, and sends distress signals up the vagus nerve. Research on H. pylori-associated gastritis has found it directly reduces the interstitial cells of Cajal, the cells that coordinate the stomach’s muscular contractions. (1) Inflammation of the lining changes how the stomach moves, not just how it feels.
What makes gastritis nausea particularly hard to live with is that it often gets attributed to something else. Pregnancy. Morning sickness. Anxiety. Food poisoning that resolves and then, strangely, doesn’t fully resolve. Many people spend years treating their nausea as its own standalone problem without anyone connecting it to the underlying inflammation driving it.
Small, frequent meals reduce the amount of time the stomach sits empty, which is often when nausea peaks.
The deeper fix is reducing the inflammation driving the motility disruption. Supporting the stomach lining, rather than just managing acid levels, is the mechanism that addresses nausea at its source rather than symptom by symptom. S-methylmethionine, the compound found in cabbage that has been studied for its role in supporting the gastric mucosal lining, may contribute to fewer nausea episodes when the lining is better supported over time. You can read more about how it works in the post on Vitamin U benefits and how S-methylmethionine supports gut health. That is a supportive effect on structure and function, not a nausea treatment.
The anxiety that comes from your gut
If you have gastritis and you also have anxiety, and the anxiety seems to get worse during flares, you are not imagining the connection.
The gut and the brain are in constant communication. The vagus nerve, which runs from the brainstem down through the chest and into the abdomen, carries signals in both directions. Most people assume it mainly sends instructions from the brain to the gut. The reverse is actually the majority of its traffic: roughly 80 to 90 percent of vagal nerve fibers transmit information upward, from the gut to the brain. (2) When the gut is inflamed, those signals change. The brain receives distress signals it interprets as threat, which produces anxiety.
There is also the serotonin question. Around 90 to 95 percent of the body’s serotonin is produced in the gut, primarily by enterochromaffin cells in the intestinal lining. (3) Gastric and intestinal inflammation disrupts this production. Less serotonin available in the gut, and the disrupted signaling that follows, has downstream effects on mood. This is not a fringe theory. A 2024 study published in BMC Psychiatry mapped the network connections between depression and anxiety symptoms in chronic gastritis patients and found that anxiety and depression occur as significant comorbidities, driven by overlapping biological mechanisms, not separate causes. (4)
I spent the first three years thinking I had a separate anxiety problem on top of the gastritis. My doctor at the time treated them as unrelated. I was sent to a gastroenterologist for one and a therapist for the other, and neither conversation included the word “gut-brain axis.” The loop continued until I started researching the connection myself.
What actually helped my anxiety most was addressing the gastritis. That sounds obvious in retrospect. When the inflammation came down, the anxiety followed. The things that helped in parallel: sleep, which I will come back to. Stress management, because psychological stress also signals through the vagus nerve and makes the gastric environment worse. Magnesium glycinate, which has evidence for both GI comfort and nervous system regulation. And accepting that during a flare, the anxiety is biological, not a character flaw, which removed a layer of shame that had been making it worse.
The eating problem
The standard advice for gastritis is to eat small, frequent, bland meals. That advice assumes you can eat. During a serious flare, many people cannot.
The double bind is specific and miserable: you feel too nauseous to eat, and the only thing that will reduce the nausea is eating. Your stomach is empty, which makes the acid exposure worse, which inflames the lining more, which makes you feel sicker. The “just eat bland food” advice does not account for weeks where every option feels impossible and you are forcing yourself through oatmeal once again.
This is what worked for me during the worst stretches, and what I have seen work consistently: the goal is soft, calorically dense, easy to consume. Not just bland. Bland alone does not solve the problem of needing to stay fed when your appetite is gone. You need food that requires minimal chewing, sits gently, and delivers enough energy and protein to keep your body functioning.
In practice, that looks like: oatmeal made with more water than usual, sometimes with almond butter stirred in for fat and protein. Soups, specifically bone broth-based ones with well-cooked vegetables. Ripe bananas. Cooked apple. White rice with a small amount of olive oil. If things are very bad, commercial liquid nutrition or even baby food is not a failure. It is a practical solution to a real problem.
The foods that made things worse during a flare, in my experience: raw vegetables, dairy (for me specifically), anything acidic, anything fried, anything cold. Cold temperature itself can trigger gastric spasm in some people with sensitive stomachs.
What is actually happening is that the inflamed lining needs time and reduced irritation to begin recovering. The food choices during a flare are not the cure. They are the management layer that keeps you functional while the lining works on healing. The repair piece is separate. I have written about that in detail in the post on how to repair the stomach lining naturally.
One thing I want to say clearly: if you are losing significant weight during a flare, or you cannot eat at all for more than a few days, this is a medical situation, not a dietary one. See a doctor. Prolonged inability to eat with gastritis can escalate.
The depression that follows
This one is the hardest to write about because it is the least validated in everyday conversation about gastritis.
When I am in a serious flare, I get depressed. Not low mood. Not feeling a bit down. Full depression: wanting to be in a dark room, no energy for anything, no motivation to do the things I know would help, no interest in anything outside getting through the day. It feels like there is no serotonin left anywhere in my system. I have not heard many people describe it this way. It is one of the reasons I am writing this post.
There are three things happening at once when this kind of depression hits.
The first is biological. Gastric inflammation disrupts the gut’s serotonin production and the vagal signaling that helps regulate mood. The brain is receiving a sustained stream of distress signals from an inflamed gut, and the neurochemistry shifts accordingly. The 2024 BMC Psychiatry study on chronic gastritis patients confirmed that depression is a meaningful comorbidity, not just something that happens to people who are upset about being sick. (4)
The second is cumulative. Chronic discomfort, disrupted sleep, reduced appetite, and constrained daily life compound over time. A single bad week is manageable. Months or years of flares, partial recoveries, and uncertain timelines accumulate into something heavier. The body is exhausted. The mind follows.
The third is isolation. Gastritis depression is not the kind of depression that comes with an obvious external explanation. There is no loss, no clear trigger. You have a stomach condition, and now you are in a dark room, and you feel ashamed of how badly you are doing over something that is supposed to be a digestive problem. That shame adds weight.
What helps: naming what is happening matters more than it sounds. Understanding that the depression has a biological driver, not just a psychological one, changes the relationship to it. Treating the gastritis itself is the strongest lever, because when the inflammation decreases the mood shift follows. Sleep is not optional during a flare. The vagal nerve regulation practices that help anxiety also reduce the biological fuel for depression. And if the depression becomes severe, professional support is not optional. This is not something to tough out alone when it reaches a certain level.
To be clear: this post is not a substitute for medical advice, and nothing in it is a treatment for depression. If you are struggling with depression and you have not spoken to a doctor, please do.
Why none of this is in the standard gastritis content
Most gastritis content online was written by people who do not have gastritis. Content marketers, medical writers summarizing clinical guidelines, AI tools summarizing other summaries. The focus is on the symptoms that show up most often in the diagnostic literature: epigastric pain, bloating, early satiety. Those are real. They are also the symptoms that are easiest to describe without first-person experience.
Nausea-dominant gastritis, gastritis-related anxiety, the eating problem during serious flares, and gastritis depression are all documented in the published research. They are just not written about in plain language by people who have experienced them. The clinical literature acknowledges the gut-brain connection. The mainstream health content mostly does not.
There is also the medical specialty problem. Gastritis is a GI condition. Anxiety and depression are mental health conditions. The two specialties rarely coordinate. When patients raise anxiety with a GI doctor, they are often referred to a therapist. When they raise the GI connection with a therapist, the therapist often does not have the tools to address it. The patient ends up bouncing between two conversations that never quite intersect.
The research has caught up. Clinical practice is slower. Until the two specialties close the gap, people with chronic gastritis need to know this connection exists so they can bring it to the table in their own medical appointments.
What I actually do
This is my current protocol, for context. Not a prescription. What works for me after ten years of having this condition.
On food: I eat every four hours. Not because I am always hungry. Because an empty stomach is consistently worse for me than a full one, and the nausea is harder to manage on an empty stomach. I avoid spicy food and alcohol. I reduce the amount of coffee and chocolate I eat.
On stress: this is the single biggest lever for me, bigger than any food change. When my stress is poorly managed, flares are more frequent and more severe. When it is well managed, I have longer stretches of feeling fine. I take sleep seriously for the same reason. Chronic sleep disruption drives inflammation and makes the gut-brain axis harder to regulate.
On supplementation: I take S-methylmethionine (Vitamin U) daily. The evidence on its role in supporting the gastric mucosal lining goes back decades and includes modern clinical trials. I make it because I use it, and I use it because nothing else I have tried addresses the lining directly the way it does. You can read the full research summary in our Global Vitamin U Research Database. I also take CBD oil, specifically for nervous system regulation, and I have found it helpful for both the anxiety layer and sleep.
On medical care: I have a gastroenterologist I see for monitoring. I recommend this. Chronic gastritis can progress, and monitoring matters even when you feel well.
A note to close
You are not making this up.
If your gastritis comes with nausea that lingers for weeks, with anxiety that shows up during flares, with stretches where you can barely eat, with depression that sits in your chest like a weight with no clear explanation: that is what chronic gastritis actually does to a body. The reason you have not seen it written down is not because it is unusual. It is because the people who usually write about gastritis have not had it.
The research says what most gastritis patients already know from experience: the condition is not just in the stomach. It is in the nervous system, the gut-brain axis, the serotonin pathways, and the cumulative toll of living with chronic inflammation. All of it is real, all of it is documented, and all of it is worth bringing to your doctor’s attention.
This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider about your symptoms and before making any changes to your treatment plan. If you are experiencing severe depression, please seek professional support.
This statement has not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
References
- Helicobacter pylori causes delayed gastric emptying by decreasing interstitial cells of Cajal. PMC, 2021. https://pmc.ncbi.nlm.nih.gov/articles/PMC8111862/
- Gut-Brain Axis in Gastric Mucosal Damage and Protection. PMC, 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5333589/
- The Mechanism of Secretion and Metabolism of Gut-Derived 5-Hydroxytryptamine. PMC, 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8347425/
- Mapping network connection and direction among symptoms of depression and anxiety in patients with chronic gastritis. BMC Psychiatry, 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11444727/

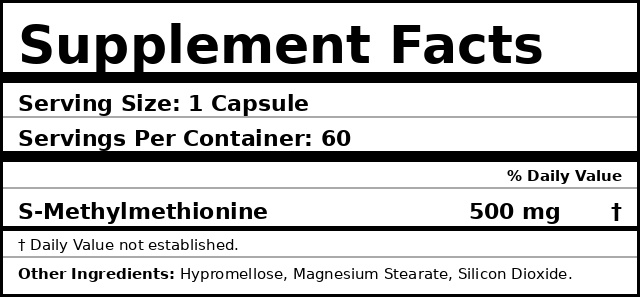
S-Methylmethionine • 500mg • 60 capsules
Vitamin U
Supports stomach lining health.*
★★★★★
$49
Free-shipping anywhere in the US
Made in USA
Lab tested 3rd-party
Capsule Vegan
Returns 30-day