I’ve had chronic gastritis for ten years.
I’m a certified holistic nutritionist, which gave me a head start when I was first trying to figure out what was happening to me. Even with that head start, I spent the first few years confused, frustrated, and lost in advice that didn’t quite fit. If you’ve been told you have chronic gastritis and you’re now Googling what that actually means at 11 p.m. on a weeknight, this is the post I wish I’d had on day one.
The name is simple. The experience is not. Chronic gastritis isn’t one bad day after a heavy meal. It’s a persistent inflammation of the stomach lining that can drag on for months or years, sometimes quietly, sometimes loudly, often without a clean explanation for why it won’t go away. For the people who live with it, the condition becomes background noise to daily life: a burning that flares after meals, a stomach that feels full before you’ve eaten much, a nausea that shows up with no warning. Some days you barely notice it. Some weeks you can’t think about anything else.
What follows is what chronic gastritis actually is, what causes it, why it tends to stick around, and what the evidence says about managing it. This is not medical advice. It is the honest version, written by someone who has been living with it for a decade.
What chronic gastritis actually is
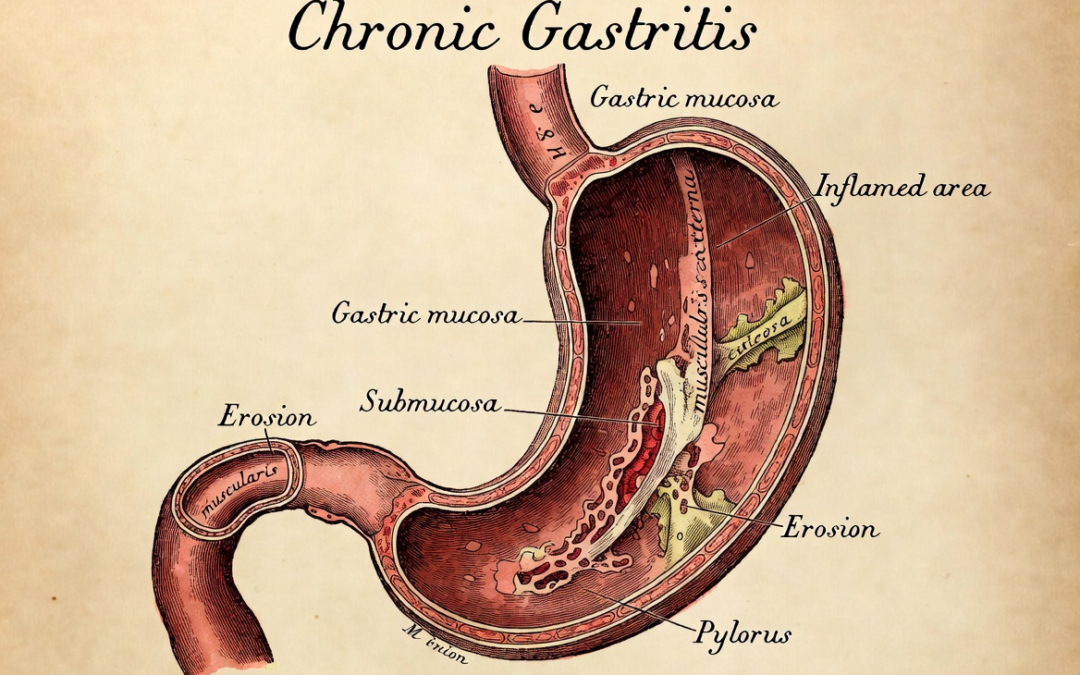
Your stomach lining does two jobs at once that seem contradictory: it produces the acid and enzymes that break down food, and it protects itself from that same acid. The mucosal lining is the barrier that makes this possible. It’s a thick, mucus-coated layer of cells that keeps the harsh chemistry of digestion from damaging the stomach wall itself.
Gastritis is what happens when that barrier gets inflamed. Acute gastritis is short-term, triggered by something specific like alcohol, a course of ibuprofen, or a stomach bug. It typically resolves in a few days once the trigger is removed.
Chronic gastritis is different. It develops gradually, often without a single obvious cause, and it lingers. The inflammation persists. The mucosal lining may thin over time. Because the damage builds slowly, many people have it for years before they get a diagnosis, or before symptoms become noticeable enough to see a doctor.
That last part is worth pausing on. Research shows that chronic gastritis is actually common in the general population, with a prevalence around 40%. A significant portion of people with it have no symptoms at all, or symptoms mild enough to ignore. The condition is often diagnosed incidentally, during an endoscopy done for something else entirely.
That doesn’t mean it’s trivial. Left unaddressed, the consequences can escalate well beyond discomfort:
Peptic ulcers are one of the most common complications. When the mucosal lining erodes far enough, stomach acid reaches the raw tissue underneath and forms open sores. These can bleed. Significant gastric bleeding from ulcers may require hospitalization.
Progressive thinning of the lining can lead to atrophic gastritis, where the stomach permanently loses its normal gland structure and its ability to produce adequate acid and digestive enzymes. In older adults, atrophic gastritis affects nearly one in two people over 70.
In some cases, the damaged cells restructure themselves into a different tissue type entirely, a change called gastric intestinal metaplasia. Doctors consider this precancerous. Research indicates that people with chronic atrophic gastritis may have a 12 to 16 times higher risk of developing gastric cancer compared with the general population.
Nutritional deficiencies are another real consequence. Atrophic gastritis (particularly the autoimmune type) impairs absorption of vitamin B12, iron, calcium, and magnesium. B12 deficiency can develop silently over years and has serious effects on nerve function and energy.
Symptoms: what chronic gastritis feels like
The symptom picture varies quite a bit from person to person, which is part of what makes chronic gastritis frustrating to live with. There’s no single defining experience.
The most commonly reported symptoms include:
- A dull or burning ache in the upper abdomen, often worse after eating or when the stomach is empty
- Bloating and a heavy, full feeling even after small meals
- Nausea, sometimes arriving without warning
- Heartburn or acid reflux
- Early satiety: feeling full after just a few bites
- Loss of appetite
- Occasional vomiting in more severe cases
Symptoms often come and go. Some people have daily discomfort. Others go weeks feeling relatively fine and then hit a flare triggered by stress, certain foods, a course of pain medication, or no identifiable reason at all. That unpredictability is exhausting in its own right.
One important thing to know: the severity of symptoms doesn’t reliably match the severity of the inflammation. Some people with significant mucosal damage have only mild discomfort. Others with relatively modest inflammation feel it intensely. A diagnosis of chronic gastritis should be confirmed by a doctor, ideally with endoscopy and biopsy, not just based on symptoms alone.
The main causes
Chronic gastritis has several distinct causes, and identifying the underlying one matters for how it’s approached.
H. pylori infection is the most common cause worldwide. H. pylori is a bacterium that burrows into the stomach lining and disrupts the mucosal barrier. It’s estimated that up to half the world’s population carries the infection, though most people never develop noticeable symptoms. For those who do, H. pylori can drive persistent inflammation that continues as long as the infection is present. Testing for H. pylori is standard when chronic gastritis is diagnosed, because treating the infection (typically with a course of antibiotics combined with acid-reducing medication) often resolves the gastritis.
NSAIDs and aspirin are the second major cause. Non-steroidal anti-inflammatory drugs block prostaglandins, compounds the body uses to maintain the stomach’s protective mucus layer. Regular use of ibuprofen, naproxen, or aspirin can strip that protection away over time, leaving the lining vulnerable to acid damage. This is a dose- and duration-dependent issue: occasional use is rarely a problem, but regular use over months or years is a significant risk factor.
Autoimmune gastritis is less common but worth knowing about. In autoimmune gastritis, the immune system mistakenly attacks the stomach’s parietal cells, the cells responsible for producing stomach acid and a compound called intrinsic factor, which is needed to absorb vitamin B12. Over time, this leads to atrophy of the stomach lining. It’s more common in people with other autoimmune conditions.
Alcohol irritates the stomach lining directly and, over time, contributes to chronic inflammation. Bile reflux (when bile from the small intestine flows back into the stomach) can also cause chronic gastritis, though it’s less commonly discussed.
Stress is a contributing factor that many people underestimate. Psychological stress doesn’t cause gastritis on its own, but it increases acid production and can weaken the mucosal barrier, making an already-inflamed stomach worse.
Why it tends to persist
People often ask why their gastritis keeps coming back or never seems to fully resolve, even after they’ve changed their diet, cut out alcohol, and taken the medications their doctor prescribed.
The underlying cause may not have been fully addressed. H. pylori, if not completely eradicated, continues to drive inflammation. NSAID use may have continued at a lower dose, or been replaced by a similar drug. Autoimmune gastritis has no cure, only management.
The stomach lining takes time to repair. Even after the trigger is removed, the mucosal barrier has to rebuild. That’s a cellular process that doesn’t happen overnight. For people with long-standing inflammation, the lining may have thinned significantly, and recovery is gradual.
Diet and stress continue to play a role. Highly acidic foods, caffeine, alcohol, and chronic stress all maintain an environment where the inflamed lining can’t recover as efficiently. Small, persistent irritants compound.
And sometimes there isn’t a clear single cause at all. Some people have chronic gastritis with no H. pylori, no NSAID history, and no autoimmune markers. The cause is unclear, which makes targeted treatment harder.
Standard treatment: what it does, what it doesn’t, and the timing gap nobody warns you about
The conventional approach to chronic gastritis typically involves one or more of the following:
Proton pump inhibitors (PPIs) such as omeprazole or lansoprazole are the most commonly prescribed option. They reduce acid production, which gives the inflamed lining less ongoing exposure to acid while it recovers. Here’s what most people aren’t told upfront: PPIs don’t work quickly. Studies show it takes 3 to 5 days before they meaningfully reduce acid levels, and 4 to 8 weeks before the stomach lining actually heals. If you start a PPI expecting to feel better tomorrow, the first week is often a frustrating wait.
H2 blockers such as famotidine are a milder form of acid reduction. They begin working within 1 to 3 hours, which is faster than PPIs, but their effect on the underlying inflammation is limited.
Antacids are the fastest option in the conventional toolkit. They neutralize stomach acid within minutes of taking them. The tradeoff: the effect lasts only 1 to 3 hours, and they do nothing to address the inflamed lining underneath.
Antibiotics are prescribed when H. pylori is confirmed, typically as triple or quadruple therapy over 10 to 14 days.
This leaves a real gap for many people: in the days or weeks it takes for PPIs to reach full effect, symptoms persist. Antacids take the edge off temporarily. And none of these options directly support the stomach’s mucosal lining, the barrier itself that needs to recover.
Some people find faster comfort from approaches that work through a protective or coating mechanism rather than acid suppression. Deglycyrrhizinated licorice (DGL) forms a soothing gel over the stomach lining and can provide relief relatively quickly, particularly around meals. Ginger tea has well-documented anti-nausea effects that can be felt within 30 to 60 minutes. Slippery elm works similarly through mucilage, a coating compound that soothes irritated tissue.
S-methylmethionine (Vitamin U), found naturally in cabbage and other cruciferous vegetables, has been studied for its role in supporting the stomach’s protective mucus layer. Clinical trials measured its effects over weeks and months, not minutes. But the mechanism (supporting mucosal barrier integrity rather than suppressing acid) is fundamentally different from how PPIs work. Some people who have switched from relying solely on acid suppressors to including mucosal-support approaches report noticing digestive comfort more readily during flares.
This is an area where the research is still developing, and individual responses vary. But understanding that fast symptom relief and long-term lining recovery are two different problems, with different tools, is a useful starting point.
What else is worth knowing
There’s a growing body of research on compounds that may support the stomach’s mucosal lining alongside or after conventional treatment.
Dietary adjustments are consistently recommended: reducing caffeine, alcohol, acidic foods, and processed sugars, while increasing easily digestible whole foods, cooked vegetables, and anti-inflammatory options like ginger and turmeric. These don’t cure gastritis but create a less hostile environment for recovery.
Probiotics have been studied as an adjunct, particularly for H. pylori-related gastritis, where strains like Lactobacillus and Bifidobacterium may improve eradication rates when used alongside antibiotics.
Demulcent herbs such as deglycyrrhizinated licorice (DGL) and slippery elm are often used by practitioners for their soothing, coating properties, though clinical evidence is limited.
S-methylmethionine (Vitamin U) is a compound found in raw cruciferous vegetables, especially cabbage, that has been studied in human clinical trials for its gastroprotective properties. Research going back to the 1950s and continuing through a 2023 clinical study found it may help support the stomach’s mucosal lining and promote digestive comfort. Some people with chronic stomach sensitivity explore it as a supportive option for maintaining stomach lining health. You can read a full overview of the human and animal research in our Global Vitamin U Research Database.
When to see a doctor
See a doctor if:
- Your symptoms have lasted more than a few weeks
- You’re experiencing unintentional weight loss
- You have difficulty swallowing
- You’re vomiting blood or passing dark, tarry stools (this needs urgent attention)
- Symptoms are significantly affecting your quality of life or sleep
Chronic gastritis can progress in some cases to peptic ulcers or, in rare instances over a long period of untreated atrophic gastritis, to more serious conditions. A proper diagnosis, which usually involves an endoscopy, is the only way to know what you’re actually dealing with.
A note from someone who has it
If you’ve read this far, you’re probably one of the people I wrote it for.
What I’ve learned in ten years is that the people who feel better are usually the ones who go looking. They get clear on what’s actually driving their inflammation. They take the medications they need but stay curious about what else might help. They support their stomach lining the way you’d support a wound: with patience, time, and the right inputs.
There is no single fix for chronic gastritis. There is a real path through it, and it usually has more than one part. A good gastroenterologist. A diet that doesn’t punish you. An honest read on what’s actually working and what’s just expensive. The willingness to keep trying things, carefully, when the last thing didn’t land.
If you’re still looking, you’re not doing this wrong. You’re doing what the people who get better tend to do.
This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider about your symptoms and before making any changes to your treatment plan.
This statement has not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
References:
1. Prevalence of Histological Gastritis in a Community Population. Digestive Diseases and Sciences, 2023.
2. Common occurrence of atrophic gastritis in an ageing population. Age and Ageing, 2025.
3. Complications of Chronic Gastritis. Pfizer HealthAnswers.
4. Gastritis. Cleveland Clinic.
5. How Long Does It Take for Omeprazole to Work? GoodRx.
6. Gastritis. StatPearls, NIH.

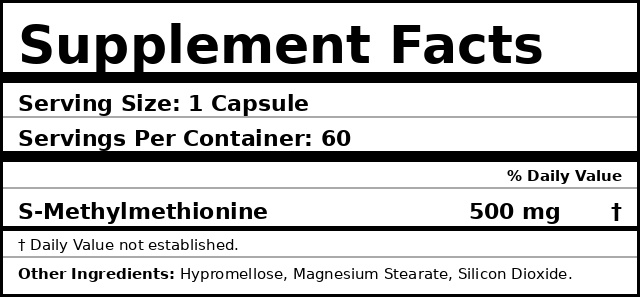
S-Methylmethionine • 500mg • 60 capsules
Vitamin U
Supports stomach lining health.*
★★★★★
Pure S-methylmethionine is the active compound in cabbage juice, studied since the 1950s. Clean formula. Made in the USA.
$49
Free-shipping anywhere in the US
Made in
USA
Lab tested
3rd-party
Capsule
Vegan
Returns
30-day